What is the value of design? Can design be valued? Is design worth investing in if you are funding a complex building for high cost workers and the public? Is design significant for Australians? The answer is a resounding yes, writes Dr Rhonda Kerr.
Architects and their clients recognise the value of design in transforming the lives of people. But it has been hard to quantify that benefit. Costs are easily identified but benefits are more elusive and are, perhaps, considered too subjective. We recognise beautiful engaging spaces but wonder and delight are not easily translated into a dollar value for potential clients and investors to appreciate.
Speaking the language of investors is key to identifying the value added by architects bringing their experience, information gathering skills and imagination to a project about people. The dollar value of architects’ creativity was able to be measured in a recent research project for stroke survivors, which compared three innovative ward designs against a standard racetrack ward design.
Stroke rehabilitation in Australia
Stroke costs Australia $15.7 billion over a lifetime including $5.5 billion in direct healthcare costs. After acute hospital care it is best practice for stroke patients to move to rehabilitation in an inpatient facility to regain cognitive and functional skills. Rehabilitation averages 23 days and has a median cost of $ 30,000 per patient. Despite survival rates for stroke improving, the annual Australian National Disability Insurance Scheme (NDIS) costs for people disabled by stroke was $1.08 billion (increasing by 38% over the year) to June 2023. Facilities for stroke rehabilitation (SR) are rarely purpose-built, and are commonly designed similarly to acute care units, despite the increased clinical focus on activity and independence, and the prolonged length of stay.
Our recent research project aimed to assess the value of evidence-based facilities in SR for patients, the health system, and the economy. The value and cost of innovative evidence-based SR ward designs were assessed compared to a standard racetrack ward design based on the Australasian Health Facility Design Guidelines. The assessment of costs and efficacy is patient-based to examine how clinical care is delivered for the benefit of the patient.
Design as an enabler of better care
The research has identified that investing in high quality architectural design delivers significant benefits to the economy and the productivity of workers.
For health facilities, designing so specialist doctors, nurses and allied health professionals can effectively deliver cutting edge care saves money for the health system, for hospitals and the National Disability Insurance Scheme. But, most importantly, it restores the capacity of patients and their carers to work and live good productive lives, the research shows.
Innovative ward designs
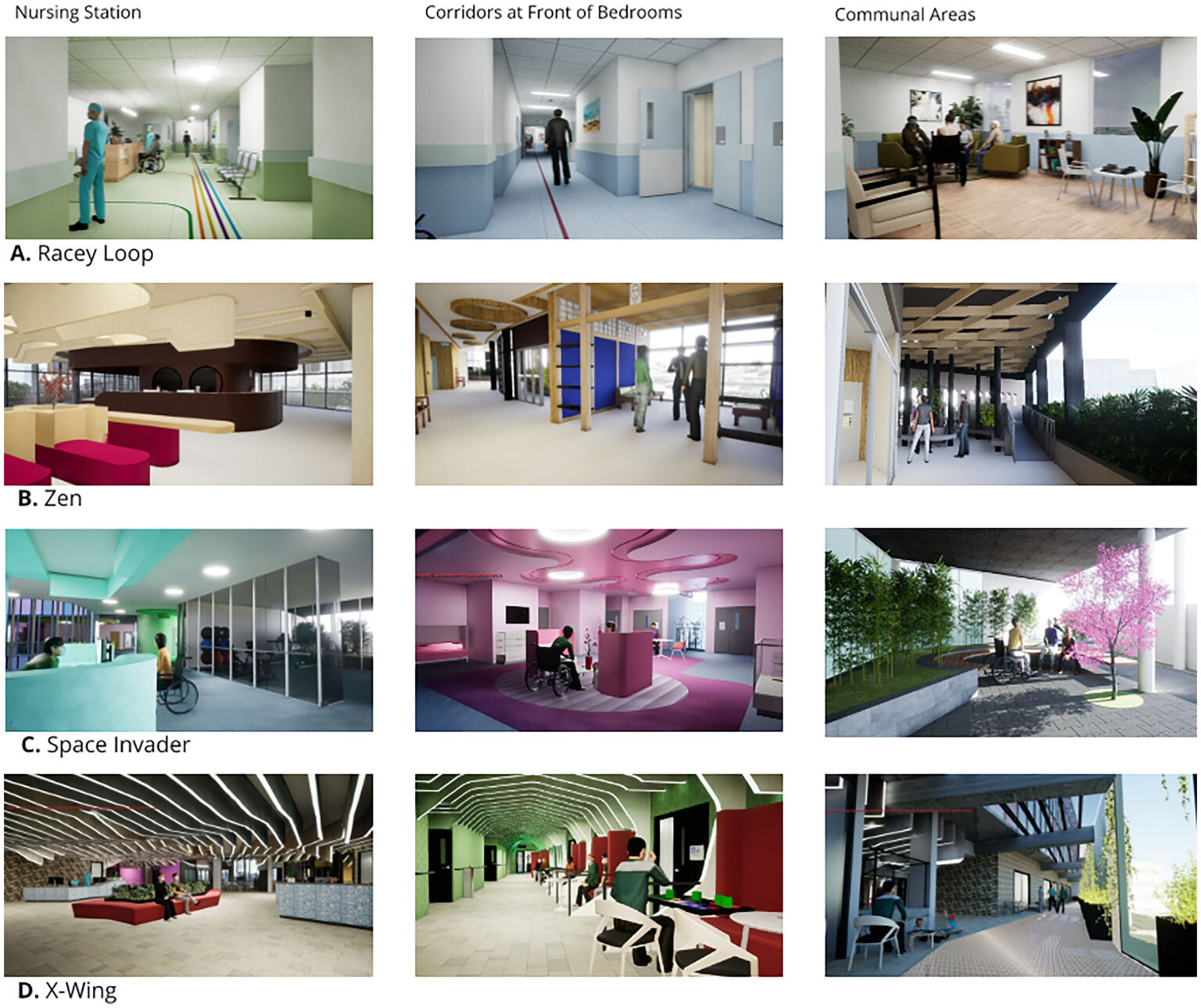
The NOVELL Redesign Living Labs approach analysed clinical research and expert advice to inform the Stroke Rehabilitation ward designs. Swinburne Architecture faculty architects, in concert with specialist clinicians, stroke survivors and researchers, developed four ward design options. When three innovative designs were compared to a standard ward design, it was evident that better patient therapies could be deployed, better patient outcomes could be achieved and economic benefits identified.
Valuing both the standard stroke rehabilitation ward design and the three innovative designs identified that for a ward of 30 beds (costing $12.77 million per annum in operating costs) innovative architectural design can:
- Achieve $3.3 million saving in hospital staffing cost (26% of operating costs p.a.)
- Deliver $12 million in benefits to the Australian and local economy
- Reduce NDIS payments of between $3.93 million and $5.4 million for every subsequent year.
How? The difference was person-centred costing. Rather than simply evaluating a building project in isolation we focused on the purpose of the building. Hospital buildings are enablers of care.
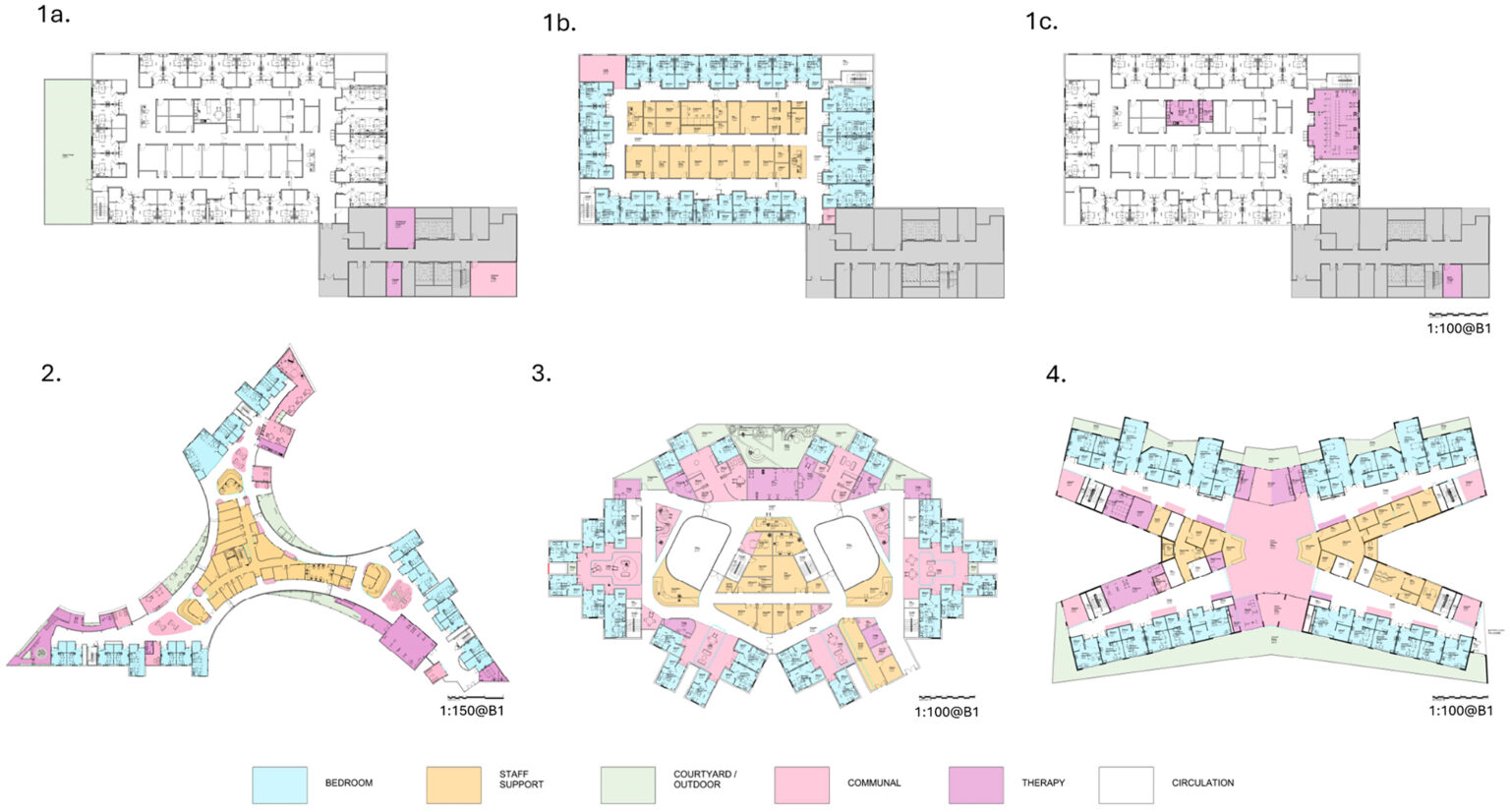
Building on a detailed review of the clinical research results, the three innovative designs had greater floor areas than the standard racetrack ward design. The innovative designs activated corridor spaces, created more communal settings and included both indoor and outdoor therapy areas for patients and clinicians. The standard design has 419m² for these activities, Zen has 4.7 times that area (1962m²), and Space Invader and X-wing have 3.5 times the area (1487m²). Total areas were 2275m² for the standard design, 2560m² for Space Invader, 2585m² for X-wing and 3295m² for Zen.
Total capital costs per patient are between $2,507 and $2,773 per patient for the four designs. Differences between the capital costs of the four designs are comparatively modest, representing between $85 and $265 per patient. However, the improved outcomes were found to be $7,500 per patient.
This study evaluated how well the designs supported effective clinical practice and enabled patient engagement. Innovative architecture facilitated clinical improvements, personal agency, cultural appropriateness, clinical support and staff retention. Importantly, innovative design allowed the integration of new technologies to enhance patient treatment resulting in shorter lengths of stay and better patient outcomes.
Conclusions
This research demonstrates the fiscal responsibility of investing in innovative architectural design to enable evidence-led innovation. Skilled architectural design proved to be an effective method for translating medical research into better patient care. It shows that assessing health facilities in terms of patient care is more important than considering the capital cost in isolation from the purpose of the infrastructure. It also demonstrates that activating inpatient facilities to meet the specific requirements of clinical effectiveness for specific patient groups was more cost effective than the standard, generic or traditional design option.
This article draws on a longer paper published in HERD Health Environments Research & Design Journal, “Economic Argument for Innovative Design From Valuing Patient-Centered Stroke Rehabilitation.” Authors include Rhonda Kerr, Ruby Lipson-Smith, Aaron Davis, Marcus White, Mark Lam, Julie Bernhardt, Juan Pablo Saa, Tianyi Yang and the NOVELL Resdesign Collaboration. It is well worth reading the full piece!

Dr Rhonda Kerr is a Health Economist and Health infrastructure Planner. She chairs the Australasian Association of Health Planners, is the Executive Director of Planning for the Guidelines and Economists Network International and is a Hon. Research Fellow at the University of Western Australia. She was honoured to be a member of the NOVELL Redesign project of the Florey Institute. Rhonda’s research focuses on capital resourcing to make healthcare more effective, sustainable and innovative.